Welcome to your medical student Emergency Medicine rotation. You may feel very familiar with emergency medicine. It is a staple of prime-time television drama, and you will have almost certainly visited the emergency department during your previous rotations. Other specialists may have given you their opinion, not always flattering, of the emergency department. We hope that while you are with us, we will deepen your understanding of emergency medicine, and help you learn skills that will help you throughout your medical career.
There will certainly be emergencies. On any shift, you could suddenly be a practical part of a team that is striving to save a patient’s life. You will learn the basics of keeping a patient alive. But you will also find that critical care is not the only part of emergency medicine. It is not even the most difficult part.
Emergency medicine deals with undifferentiated illness. By the time a patient reaches the inpatient ward, they often have a label of pneumonia, angina or appendicitis. In the emergency department they had shortness of breath or abdominal pain. Emergency medicine is a diagnostic specialty. Most of our time is spent trying work out who is really sick, without taking too much time or ordering unnecessary tests. The most stressful aspect of emergency medicine can be deciding whether to send home a patient with a headache that is probably a migraine, but just might be a cerebral haemorrhage.
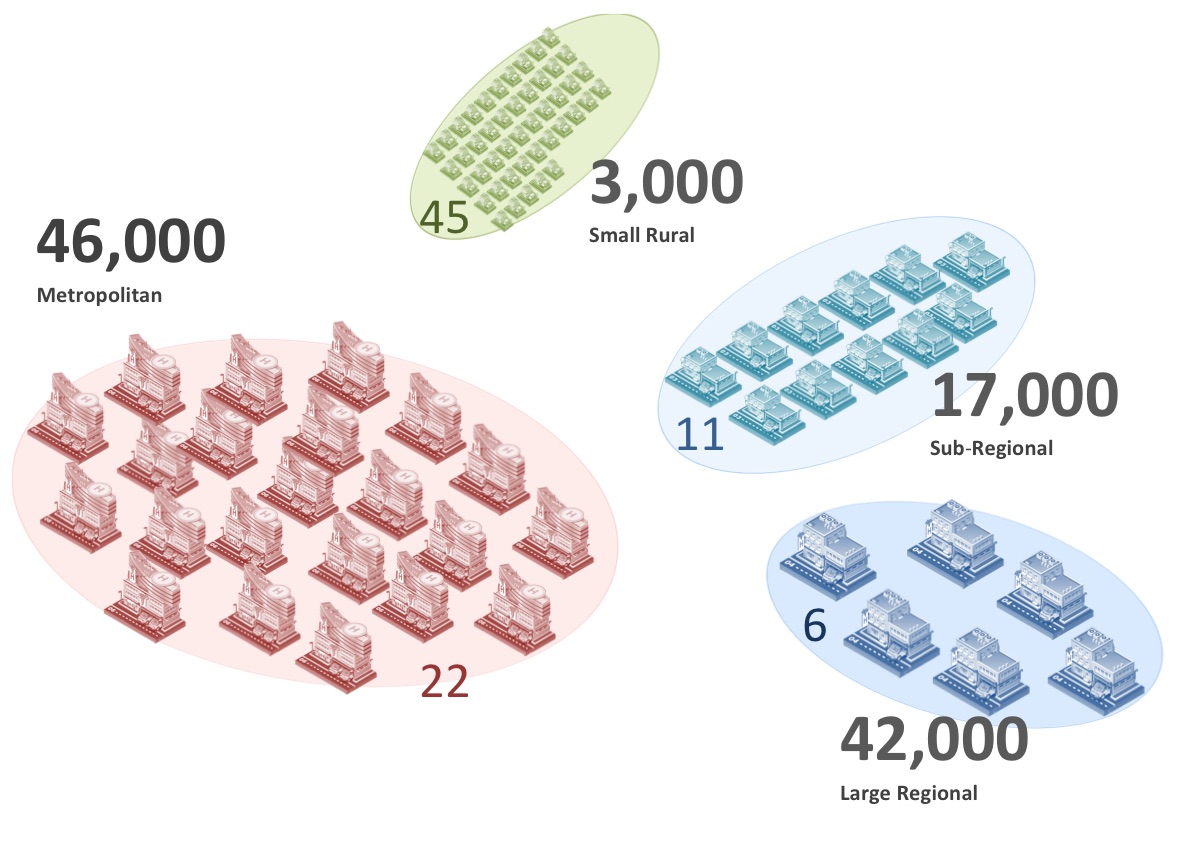
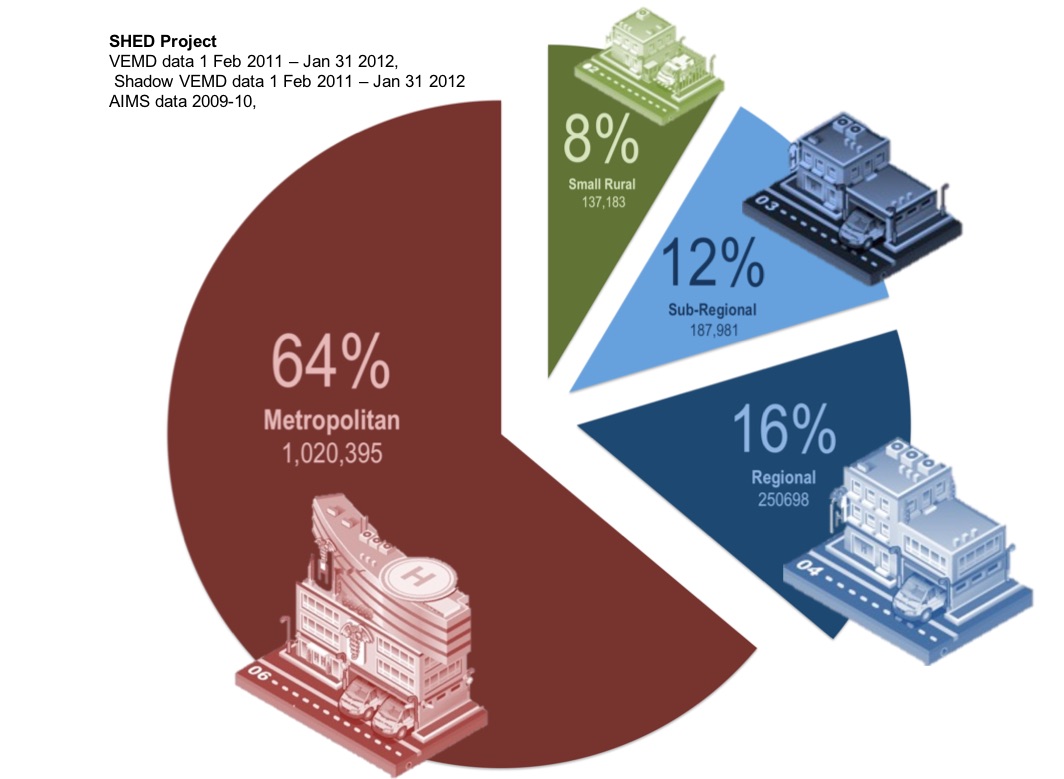
The emergency department is also where the hospital meets the community. On a single day you may speak to general practitioners, specialty units, community teams, health administrators, paramedics and the police. The stresses on the health system are often most obvious here. You will see how people move between various areas of health care. You will see how they can end up in the emergency department when they fall through the cracks. You may also see how the stresses of shift work and time pressures affect you.
In these few weeks, you will perform many practical skills for the first time. Minor procedures are common in the emergency department. You should have practiced these tasks in the skills lab, but performing procedures on real people is different; they feel pain, they move, their anatomy is unique, and they may ask you to stop. Practicing procedures on patients will make you feel uncomfortable. To become a practical doctor you must become comfortable with being uncomfortable. We will be here to help. You are part of the team, and performing procedures, if consent is given, that the patient needs. It gets easier. You need to become comfortable with the basic skills, so that when you are an intern you can become uncomfortable again with even more advanced tasks.
So welcome again to your emergency rotation. It might not be what you expect, but it may be what you need.